Understanding & Overcoming Anorexia Nervosa
Please download this PDF version of Understanding & Overcoming Anorexia Nervosa
Viewed from an evolutionary perspective, individuals and their families need not shoulder the blame for anorexia nervosa. Rather, understanding the challenging biological changes can help families and clinicians work together to beat it.
Anorexia nervosa is the most homogenous psychiatric disorder, yet its stereotyped symptoms are the opposite of what one expects of a starving person. Although at least 15% below normal weight, people with anorexia feel energetic and reject foods that used to tempt them. This mysterious illness has been attributed to psychological problems in the individual or their families, or to biological dysfunctions.
Blind to their own bodies
As strange as it may seem, when people first develop anorexia nervosa they may not be aware that something is wrong because their bodies send them false signals. For example, underweight anorexics literally cannot see that they are too thin.
This brain-imaging picture shows the pattern of activation of the visual cortex when women look at other’s bodies and when they look at themselves(1). As these pictures dramatically illustrate, when people with anorexia tell us “I just can’t see it,” they are telling the truth. The visual cortex is literally blinded to their own body contours while the brain region responsible for body image is hyperactive, seamlessly filling in the blank with a fattened-up version. This odd blindness happens only for an anorexic’s own body, and only when he or she is underweight(2).
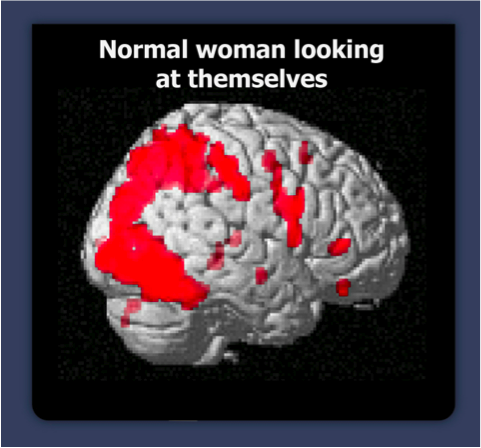
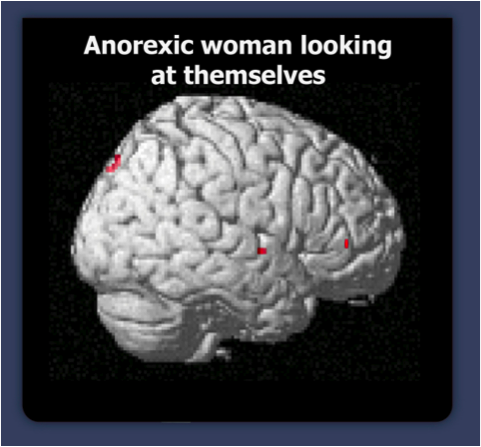
Reproduced with permission of the author from: Mondraty, N. Paper presented at The International Conference on Eating Disorders, Baltimore, MD, June 2007.
What is the anorexic brain up to?
This isn’t the only odd thing the anorexic brain does. Deep in the brain, an ancient region, called the hypothalamus, does something very odd. The hypothalamus monitors nutritional status and manipulates our appetite to get us to eat; normally when people are starving, it turns up hunger signals so they can think of little else, and it keeps satiety (fullness) signals low, so that if food becomes available, they can gorge.
Normally when people are starving, the brain’s rewards for eating are tuned up high to encourage the search for food. For example, the body turns up opiate receptors, making eating feel like an addict’s fix. It enhances cannabinoid receptors, making food taste like you’re stoned. Dopamine, the brain chemical that plays a key role in orgasm and in addictions, surges when a starving person eats. If it sounds like eating when starved releases a veritable pharmacopoeia of street drugs, you are right. Most addictive drugs exploit reward systems that first evolved to insure that animals eat.
While some brain changes increase the rewards for eating, others change what we decide to do. We assume that we are in control of our eating, but dieters know there is more to the story. Like hunger for air or water, hunger for food can irresistibly alter the will of even the strongest dieter, so that eventually a person will decide to eat.
But this system is altered in those with anorexia nervosa, so that starving people can decide not to eat. It accomplishes this by making changes at every level of the body’s powerful energy regulation system(3). The anorexic hypothalamus turns many hunger signals down and increases satiety signals, so that people with anorexia feel repelled by food and get full after small meals. Satiety signals are also turned up all through the gut, so that people with anorexia get full quickly. In the brain’s reward centers, opiates, cannabinoid enhancers, and dopamine receptors are turned down, so that food tastes flat and eating is unrewarding.
In the brain’s emotion circuits, anorexia produces anxiety and guilt about eating, and pride when resisting hunger; anorexia makes a starving person believe that it is vitally important to control his or her appetite. Yet, at the same time, two of the master hunger signals in the hypothalamus are also turned as high as in normal starvation so that people with anorexia find themselves thinking constantly about the food that that they cannot bring themselves to eat.
Anorexic attitudes and feelings have long been seen by doctors and therapists as dieting run amok. According to the Diagnostic and Statistical Manual of Mental Disorders, anorexia nervosa is the result of a “relentless pursuit of thinness” and “refusal to maintain a normal body weight” (italics added). Anorexics are assumed to be vain and neurotic — “starving for attention” or “on a hunger strike” — and their parents are suspected of being controlling and critical.
There is no scientific evidence for those assumptions (4). Careful studies have found no evidence for emotional problems specific to anorexia in the affected families, and the typical anorexic, before the illness, was hard working, high achieving and conscientious.
There are a number of other facts that do not square with the idea that anorexia nervosa is caused by psychological issues. Anorexia nervosa is genetic. Researchers have identified multiple genetic changes linked to anorexic attitudes and to altered appetite and activity regulatory molecules; significantly, these genes are turned on when body weight drops (5). The core symptoms of anorexia–difficulty eating, hyperactivity and body image distortion–do not vary across individuals, historical era, sex, age, and culture (6), which is expected if anorexia symptoms were a symbolic response to personal conflicts. Instead, the core symptoms are consistent with a biological response to starvation.
Finally, what anorexics are able to do–keep their weight 15% or more below normal–is very remarkable biologically. Energy regulation researchers claim that it is normally impossible for individuals to do this for long.
Why do we think that a 14-year-old girl can willfully resist hunger when adults cannot? Neuroscientists (and parents) know that the part of the brain that helps us exert self-control is not fully mature until people are in their mid-twenties.
In fact, anorexic food refusal is not due to will power. When people with anorexia try to recover, they find that body and mind fight them. As Kari Chisholm wrote in Hungry Hell “It took a lot of self-control to lose the weight, but even more to gain it back.”
Adapted to flee famine
Only those who have the genetic ability can develop anorexia nervosa if starving or very underweight. But, why do some people carry such genes?
At one time in human history the symptoms of anorexia nervosa must have been selected as a useful response to the threat of death by starvation.
Normally, starving people are ravenous, tired and demoralized; they conserve energy and focus on finding food. But consider the challenges that faced our hunter-gatherer ancestors in the Pleistocene, only a few tens of thousand years ago. When nomadic foragers had depleted local food, and mountain ranges, oceans or deserts barred farther travel, normal responses to starvation (lethargy that conserved energy, hunger that motivated single-minded search for food, and awareness that they were emaciated) would have interfered with making a difficult and frightening journey.
If some starving foragers were able to ignore their hunger and energetically move, they might have survived at higher rates than those who stayed put (7). For these special members of the group, self-deception about body image, fat stores, and about how depleted their bodies really were would have provided the optimism to travel. Personality traits of conscientiousness and self-control (both associated with anorexia today) could also have helped explorers persist on desperate journeys with little hope of success. I called this evolutionary explanation of anorexia nervosa the adapted-to-flee-famine hypothesis.
The March of the Penguins
The adapted-to-flee famine hypothesis may sound impossible to prove, but many kinds of evidence support it. Nature gives many species the ability to develop anorexia (lack of hunger)[1] when it would compete with other life tasks. If you saw the movie March of the Penguins, you know that Emperor penguins must become anorexic to breed; males may lose half their body weight while incubating! Other species also reduce eating to migrate or to defend a breeding territory.
Like humans, rats and pigs evolved as omnivorous foragers, and they also become anorexic and energetic when starving. Animal researchers attribute this behavior to the animals’ instinctive attempts to leave food-depleted areas (8). Pigs bred for leanness are vulnerable to developing anorexia if they lose additional weight from the stress of maternal separation or bullying from other pigs. In the lab, if given exercise wheels, starving rats ignore their food to run. Although rats normally run less than a mile a day, these frantic animals clock up to 12 miles a day as though they were trying desperately to get somewhere. If allowed, these caged rats eventually die of self-starvation.
Is there any evidence that prehistoric people really did travel long distances? In the last 50,000 years humans traveled to every habitable part of the earth. Before historic times humans were already more widely distributed than any other mammal. Furthermore, these early humans were such effective hunters that they repeatedly overhunted native prey populations. This led to local famine and the need to migrate in search of new food (9). Only those people and groups that migrated colonized new worlds. The ancestors of today’s anorexia patient may have been the ones who scouted ahead for better lands for the tribe.
Most prehistoric hunter-gatherers did not make it to the next continent. As few as 500 of the people who left Africa gave rise to the modern populations of the rest of the world. According to molecular genetics research, the founding population of American Indians may have only been 70 individuals (10). And, bands with anorexic members were apparently among the founders. Anorexia nervosa is extremely rare in Africans; it is more common in Europeans and Asians, and appears to be most common in Native Americans who have traveled the farthest from Africa (11).
Extreme Sport
Anorexics report feeling they are not supposed to eat. They feel ashamed of giving in to hunger. It feels right to them when they restrict food and exercise, and it is remarkably difficult to reason with them about their beliefs. Although these behaviors seem to be chosen by the patient, patients talk of being “taken over” by the anorexia. It is striking that people as different as reservation Indians, middle school girls, underweight boys, and elderly women express the same bizarre thoughts and feelings when they develop anorexia.
These anorexia attitudes seem illogical to non-anorexics, but we accept, and even laud, athletes who express similar dogged commitment to practicing their sports. This may be a similar situation to anorexia. It is no longer necessary to hunt food and physically defend one’s family, but most people still feel compelled to practice athletic skills, encourage their children to practice, and deeply enjoy watching athletic contests. Our attitudes toward sports are probably an evolutionary holdover from a time when one person’s prowess in throwing or running could save an entire tribe from starvation or in battle (7). We even call certain athletes heroes. I suspect that both athletes’ attitudes toward enduring hardship and anorexics’ attitudes toward resisting hunger were selected because they helped our Pleistocene ancestors survive.
But why would anorexic attitudes get triggered today, when there is plenty of food? We might as well ask why people become obese when there is no need to store extra fat. If your ancestors survived frequent famine by storing fat in the good times and if this ability is inherited, the hypothalamus can make your body store extra fat despite your conscious awareness of plenty.
The hypothalamus, which attends to energy and water balance and other basics of survival, doesn’t get information from the thinking part of the brain, but rather by monitoring the blood. Then, according to rules dictated by evolution, it initiates changes in energy metabolism, appetites, attitudes and behaviors to get the body what it needs.
This powerful energy regulation system is the reason dieters eventually regain their lost weight. We can try to tell our body that there is no reason to store this extra fat, but the hypothalamus can’t hear us. Similarly, if your ancestors survived famine by migrating, the hypothalamus reads very low body fat as the signal to pull up stakes and move. It then deceives you about your fat stores, compels you to control your appetite, and drives you to move. You can develop anorexia nervosa if you lose enough weight for any reason. The hypothalamus does not care whether the weight loss is from illness, over- activity or dieting.
Why do anorexic females outnumber males?
It is commonly assumed that girls and women are more susceptible to anorexia because they are trying to look like anorexic-level thin models. Female anorexics have always outnumbered males — even when thin was not in. Although our culture’s idealization of unhealthy levels of thinness certainly leads to dieting, and it starts some on the path to anorexia and other eating disorders, it turns out that thin standards are not the primary reason for the sex difference. In fact, until the 1930s, historical accounts did not even describe a “pursuit of thinness” as the motivator for anorexia nervosa. Historically, fasting was associated with religious piety, not appearance. Diaries and other firsthand accounts show that many people considered holy in history (then also mostly women) displayed typical anorexia symptoms of food restriction, over-activity, and denial of starvation, although they did not express modern anorexics’ fear of fat (12).
Before puberty as many boys as girls develop anorexia. After puberty nine females develop anorexia for every male. Researchers have found a genetic mutation on an estrogen receptor that turns on the capacity to develop anorexia at puberty in girls (13). The frequency of this genetic variant indicates that, when this gene was selected, it was more adaptive for reproductive females than for prepubescent girls, boys or men to develop anorexia.
Again, the life of nomadic hunter-gatherers may explain why. If a man and woman encountered another band while looking for food, the woman was more likely to survive. Even if captured she would likely reproduce. Thus it was generally safer for reproductive females to travel. Molecular genetic research has discovered that females have indeed migrated farther than males in our evolutionary past. Female rats also develop anorexia sooner than males, perhaps for the same evolutionary reasons.
But is it really likely that hunter gather bands would allow young women to scout for food? Weren’t those cultures even more sexist and rigid about females’ roles and activities than out own? Actually, according to anthropologists, girls and women have always helped to provide food for their families. Hunter-gatherer societies were actually more egalitarian and open to women’s full participation than agricultural and state societies.
But, I think the most compelling evidence that young women could have led their starving bands is the story of Joan of Arc. She was an illiterate peasant girl in medieval France, a feudal, patriarchal culture. Yet, princes and generals followed her. Joan had all the classic anorexia symptoms: she was very thin, famously ate abstemiously, had incredible energy and did not menstruate.
JOAN OF ARC: SHE GAVE EVERYTHING
Joan was athletic, tough and courageous. “She came from nowhere and gave everything,” biographer Mary Gordon observed. Because “she knew herself right and fully able and the chosen of the Lord,” she was able to convince the French Dauphin to give her command of a troop of soldiers. According to another biographer, Marina Warner, her “glorious recklessness” inspired men to follow her. She ignored hunger and fatigue, and she drove herself to punishing physical activity. To lift the siege of Orleans, Joan and her soldiers traveled 350 miles in eleven days, crossing six rivers while eluding their enemies. During the first battle, when she was shot above the breast by an arrow, the French commander assumed the battle was over. But, Joan refused to retreat. She prayed briefly, remounted her horse, and took up her standard. The English fell back in awe; the French soldiers rallied to take the town.
Joan of Arc’s extraordinary courage, even when wounded and outnumbered, inspired her followers to a string of improbable victories. Gordon tells us, “The effect that Joan had on the weak and vacillating Charles is a kind of metaphor for her effect on the whole kingdom of France. Like its leader, the realm was demoralized, depressed, and divided against itself. … Suddenly, a young, brash creature appeared from the countryside.” In those desperate times France needed a fearless leader whose zealous belief could inspire hope.
Joan of Arc’s physical energy probably came from her anorexia, but she understood her extraordinary abilities in the context of what she saw as God’s will for France. Pleistocene foragers would have understood their anorexic abilities in the context of scouting for food. Today’s anorexics understand them in terms of pursuit of thinness, a “hunger strike,” or need for control.
Burned Alive
People with anorexia nervosa often run for miles on very little food. Can anorexics somehow defy the first law of thermodynamics, pulling energy from nowhere?
No. Although anorexics feel strong and fat, this is an illusion. If anorexia nervosa becomes chronic, modern sufferers, like St. Joan, are eventually burned alive by their own bodies. The starving body cannibalizes its own muscles, heart and organs. Anorexics suffer kidney failure, heart failure or seizures, all the while explaining that they cannot bear to eat. Over time people with active anorexia become shrunken and wasted. The bones, drained of calcium, are so fragile that one woman I worked with broke her hip throwing a bowling ball; another’s ankle snapped when she stepped off a curb. Even in the short run anorexia nervosa compromises health. If the disorder persists for over four months it diminishes a growing child’s height.
If anorexia nervosa goes on too long, most people eventually begin bingeing and purging. Researchers used to think that different personality types led to bulimia or to anorexia, but it now appears that bulimia often accompanies or follows anorexia, probably because normal adaptations to starvation — ravenous hunger and ability to gorge — break through from time to time and people find themselves binge eating. If the anorexic then vomits, fasts, or exercises to undo the eating binge, these remedies perpetuate the neuroendocrine signals that cause uncontrollable hunger and establish a vicious cycle of bingeing and purging.
When anorexia nervosa becomes chronic, people exhaust their medical insurance benefits, their friends, families, and themselves. Active anorexia ultimately leads to such a miserable life that the risk of suicide is 50 times normal. In 1991 a Dutch court dismissed charges against a physician who had assisted in the suicide of 25-year-old woman with a 16-year history of anorexia because they concluded “the woman had been suffering unbearably with no prospect of improvement.”
Anorexia demands that everything be sacrificed; friends, spouse and children take second place to the need to exercise, avoid eating, or to purge food already eaten. Loved ones take relapses personally, while explanations invoking anorexic’s “need for control” make families back away from the patient. The assumption that victims refuse to maintain a normal weight leads many to blame victims for their plight. In today’s society, anorexia nervosa makes its victims secretive, lonely, and frail.
Trapped by ANA
A typical first-time anorexic is a 14-year-old girl who has always been lean and active. Why are 14-year-old girls more vulnerable? At puberty girls have attained their adult height but have not filled out. They are typically leaner than at any other time in their lives. Now, like the lean-bred pigs described above, these “beanpoles” are at risk of developing anorexia nervosa if they lose any weight for any reason, whether from illness, athletics, or dieting. Some of my young patients are adamant that they do not have anorexia nervosa because they were never trying to lose weight. But, sadly, they have all the other psychological and neuroendocrine symptoms, including inability to see how thin they are, difficulty eating, and drive to exercise. Anorexia traps some for years.
However, anorexia is not confined to youth. If you have the genetic ability to develop anorexia, it can be triggered whenever body fat drops too low. Dangerous times occur around life transitions that disrupt eating or that inspire dieting: the first years of college, pregnancy and childbirth, school reunions, divorce or death of a spouse, and loneliness or illness in old age.
Because anorexia imbues an ordinary mortal with seemingly supernatural powers, it can also reassert itself when one’s sense of self is threatened. If a person feels out of control in his or her job, marriage, or parenting, dieting to an anorexic weight can make the person feel in charge again. Anorexic thoughts and attitudes get fit into whatever psychological issue the person has; this is probably the reason that eating disorders specialists remain convinced that psychological issues cause the disorder.
“Parents are the worst attendants”
In 1874 Frances Gull, the physician who gave anorexia nervosa, its name, noted that when patients returned home they often lost the weight they had gained in the hospital. He concluded that “parents are the worst attendants” for their anorexic children. This pattern of blaming parents for relapses and for the disorder itself has continued. The most important twentieth century theorist, Hilde Bruch wrote that anorexics were “engaged in a desperate fight against feeling enslaved and exploited” by their mothers. Clinicians advised “parent-ectomies.” Parents were to stop putting pressure on the child to eat and let the professionals do the work. Even today, most clinicians still assume that food “refusal” represents a struggle for independence. Clinicians may suspect that an absent father drives his daughter to “starve for attention,” or that a mother is so controlling that food is the only thing her daughter can take charge of.
Blaming parents turned out to have cruel and sometimes deadly effects. Some families were seriously damaged, and some children, alienated from loved ones, failed to recover. In Slim to None: A Journey through the Wasteland of Anorexia Treatment Gordon Hendricks used his daughter Jennifer’s journals to chronicle the treatment that ended with her death. The father’s love was labeled incestuous, the mother’s as competitive, and the parents were counseled to keep their distance. The therapist was so convinced that Jennifer’s symptoms were symbolic that she undermined the work of a dietician. After ten years battling the illness, Jennifer died alone.
Today parents have clearly been exonerated. Multiple population studies failed to find the hypothesized relation between family pathology and developing anorexia. Parents of anorexics run the gamut of parenting abilities and attitudes, but as a group they are no more controlling, critical, or absent than other groups of parents. Recently genetics researchers studying identical and fraternal twins concluded that family environment has a “negligible” effect on whether a child will develop anorexia (14). We now know that parents can no more make their children anorexic than they can make them autistic or schizophrenic; these are all biological illnesses.
But why were parents supposedly bad at taking care of their children with anorexia? One reason may be the fact that the parents are doing what a good parents does: listening. Learning to read your baby’s cues about being hungry or full is one of the first skills good parents develop. Forcing more food on a sated infant is normally bad parenting. An illness that tricks a child into believing that she is full puts the parent in the unnatural position of not listening. I think that parents can be “bad attendants” exactly because they are so sensitive to their child’s anguish, and for the person with anorexia, eating can be excruciating.
Anyone who has tried to beg, coax, and cajole an anorexic to eat knows anorexia’s certainty, misery, and intellectualization first-hand. Loved ones get the full brunt of anorexia’s desperation. We are dealing, after all, with the kin of Joan of Arc, descendants of people who — with self-control and single-mindedness — ignored their hunger and survived. Who could stand against Joan of Arc? Not her mother or father. Her brothers joined her cause.
Still, if your child were terrified of shots but needed of them, you would soothe and support her while she got the needed medicine. Recovered anorexics say that “eating through the fear” was the hardest thing they have ever done. When loved ones have anorexia, our job is to help them tolerate the acute distress of defying the anorexic body’s demands. We acknowledge their anxiety and applaud the courage it takes to eat despite it.
It takes a village
Humans are deeply social, and when anorexia evolved, people lived in groups bound together by ties of blood and responsibility. Anorexia nervosa was probably more easily “switched off” in that group context. Hunter-gatherer societies share food. When more food becomes available after famine, thanksgiving and ritual feeding of one another accompany breaking the fast. Because anorexia evolved in the context of interdependent groups, the help of friends and family may be vital to recovery — part of the process of dealing with anorexia that our modern world has forgotten.
It is likely that anorexics were a minority in most groups; this is based on its current prevalence. This could have worked to everyone’s advantage. When resources were depleted and the tribe despaired, an anorexic’s energy, optimism, and grandiosity could mobilize the other members to heroic marches. When a starving tribe reached a new hunting/gathering ground, support by the majority non-anorexic members would in turn have helped the anorexic member(s) to begin eating again. Today most people who have recovered attribute their recovery to loved ones’ support.
My body is trying to migrate
For 800 years sufferers of anorexia nervosa have been seemed to be seeking control in their lives. For the anorexic saints it was control of bodily appetites. For Victorian anorexics it was supposedly control of sexuality. In the last half of the twentieth century it is assumed to be control of body size or personal autonomy.
But for you, struggling with this illness in your family today, focus on control becomes a trap. You can replace the mantra “It’s the only thing I can control” with “My body is trying to migrate,” and with this new insight learn to heal and remain well throughout a full and productive life. Patients and their families are not helpless against the power of anorexia; in fact, with knowledge of the illness, they have the tools to beat it.
[1] The word “anorexia” comes from the Latin a = not and orexia = hunger. The term is used as a shorthand for the human eating disorder, anorexia nervosa, and is also used to refer to lack of hunger in animals.
References
- N. Mondraty, in International Conference on Eating Disorders (Academy for Eating Disorders). (Baltimore, MD, 2007).
- A. Wagner, M. Ruf, D. F. Braus, M. H. Schmidt, Neuroreport 14, 2193 (Dec 2, 2003).
- A. Inui, Mol Psychiatry 6, 620 (Nov, 2001).
- J. Hebebrand, R. Casper, J. Treasure, U. Schweiger, Journal of Neural Transmission 111, 827 (Jul, 2004).
- R. A. Adan, T. Vink, Eur Neuropsychopharmacol 11, 483 (Dec, 2001).
- P. K. Keel, K. L. Klump, Psychol Bull 129, 747 (Sep, 2003).
- S. Guisinger, Psychol Rev 110, 745 (Oct, 2003).
- W. F. Epling, W. B. Pierce, International Journal of Eating Disorders 5, 475 (1988).
- J. Diamond, Science 287, 2170 (Mar 24, 2000).
- J. Hey, PLoS Biol 3, e193 (Jun, 2005).
- M. Crago, C. M. Shisslak, L. S. Estes, Int J Eat Disord 19, 239 (Apr, 1996).
- R. Bell, Holy Anorexia (University of Chicago Press, Chicago, 1985), pp.
- K. L. Klump, K. L. Gobrogge, International Journal of Eating Disorders 37 Suppl, S43 (2005).
- C. M. Bulik, L. Reba, A. M. Siega-Riz, T. Reichborn-Kjennerud, Int J Eat Disord 37 Suppl, S2 (2005).
This is perfect. This makes perfect sense to me and I have personally found it very helpful in my own recovery to be aware that the traits/symptoms/characteristics are all simply trying to push me to find food/eat/regain weight. (I came to my own conclusion because of my experiences, which strongly suggested that it was an adaptation to a shortage of food. The probability that my traits, seemingly so perfect for regaining weight outside of a modern setting with cultural influences about food/body image, were adaptations to a famine was approx 10,000 to 1 in my head).
Recognizing that it was an evolutionary advantage and adaptation also made me feel OK about having it and so I wasn’t in denial.
Additionally it has also been helpful I think for me to understand the exact mechanism of thought process i.e. any thoughts will get ‘stuck’ and ‘assumed’ then get compulsively continued. (The perfectionism trait attributed to ‘anorexics’ is created by this thought process). This mindset would have been beneficial in an evolutionary sense by making the subject get ‘stuck’ on the thought of finding food/eating food and repeating the process compulsively, but in modern cultures the subject can ‘assume’ and get ‘stuck’ on many unhelpful things eg reasons not to eat etc. Knowing this thought process explained why some of my thoughts/behaviors were irrational, and has made me aware and cautious of that happening.